關於子宮內膜癌, 術後放射線治療的論文非常多, 以下一一來整理
1. GOG 99: 有子宮肌層 且/或 occult cervical stroma侵犯(定義三個risk factor : grade II/III, LVI, outer 1/3 myometrial invasion, 定義 high-intermediate risk pts 為(1) age>70 with 1 risk factor (2) age >50 with 2 risk factor (3) any age with 3 risk factor; 其他收案病人不符合high-intermediate risk 的都定義為 low-intermediate risk), 去做TAH/BSO, pelvic, P-A LN sampling, 和 peritoneal cytology, 之後分成 whole pelvis RT(50.4Gy) v.s 觀察, 發現WPRT 可以改善 2-year cumulative incidence of recurrence (12%->3%), 其中high-intermediate risk(26%->6%), low-intermediate risk(6%->3%), OS在兩組沒差(但是power不夠...)
2. PORTEC-1: PORTEC為post operative radiation therapy in endometrial carcinoma的縮寫, 收案條件為stage-1 endometrial carcinoma (grade 1 with deep [≥50%] myometrial invasion, grade 2 with any invasion, or grade 3 with superficial [<50%] invasion), 去做TAH/BSO without lymphadenectomy, 隨機分成EBRT(46Gy) v.s. observation, EBRT reduce 10 year Loco-regional recurrence(14% to 5%), 10-yr OS 沒差
3. PORTEC-2:
reference:
1. Keys, Henry M., et al. "A phase III trial of surgery with or without adjunctive external pelvic radiation therapy in intermediate risk endometrial adenocarcinoma: a Gynecologic Oncology Group study." Gynecologic oncology 92.3 (2004): 744-751.
2. Creutzberg, Carien L., et al. "Surgery and postoperative radiotherapy versus surgery alone for patients with stage-1 endometrial carcinoma: multicentre randomised trial." The Lancet 355.9213 (2000): 1404-1411.
3. Scholten, Astrid N., et al. "Postoperative radiotherapy for Stage 1 endometrial carcinoma: long-term outcome of the randomized PORTEC trial with central pathology review." International Journal of Radiation Oncology* Biology* Physics 63.3 (2005): 834-838
2019年5月28日 星期二
2019年5月27日 星期一
[食道癌] Cross study
Cross study 是一篇非常有名的食道癌研究,改變了食道癌的治療方法, 讓大家知道在locally advanced esophageal cancer, neoadjuvant CCRT + surgery是一個可行的治療
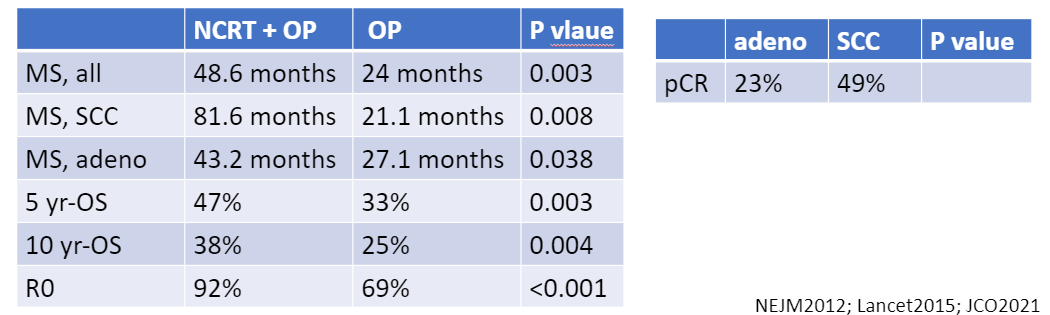
其研究內容如下, resectable esophageal ca or esophagogastric junction cancer (clinical stage T1N1M0 or T2–3N0–1M0), 分成 neoadjuvant CCRT(41.4Gy/23Fr + carboplatin + paclitaxel) + surgery v.s. surgery alone, 結果發現加上neoadjuvant CCRT 明顯改善 Median Survival (49m v.s. 24m), 非血液學的副作用在兩組沒有差別, 手術R0 resection(92% v.s. 69%, P<0.001), CCRT組的ypCR有29%, 其中pCR 在 adenocarcinoma (23%) versus squamous-cell carcinoma (49%) (P=0.008)
後來在2015年在lancet 發表長期追蹤的結果(median follow-up = 84.1 months), 確認不管是在adenocarcinoma or squamous carcinoma, 做neoadjuvant CCRT 都對OS 有幫助!
2021年又發表了十年長期追蹤結果(median follow-up:147 months), 發現neoadjuvant CRT 有比較好的 overall survival (hazard ratio [HR], 0.70; 95% CI, 0.55 to 0.89); 而且這個效應跟時間無關; 10年的overall survival benefit 是 38% v.s. 25%
MS = median overall survival; OS = overall survival
reference:
1. van Hagen, Pieter, et al. "Preoperative chemoradiotherapy for esophageal or junctional cancer." New England Journal of Medicine 366.22 (2012): 2074-2084.
2. Shapiro, Joel, et al. "Neoadjuvant chemoradiotherapy plus surgery versus surgery alone for oesophageal or junctional cancer (CROSS): long-term results of a randomised controlled trial." The lancet oncology 16.9 (2015): 1090-1098.
其研究內容如下, resectable esophageal ca or esophagogastric junction cancer (clinical stage T1N1M0 or T2–3N0–1M0), 分成 neoadjuvant CCRT(41.4Gy/23Fr + carboplatin + paclitaxel) + surgery v.s. surgery alone, 結果發現加上neoadjuvant CCRT 明顯改善 Median Survival (49m v.s. 24m), 非血液學的副作用在兩組沒有差別, 手術R0 resection(92% v.s. 69%, P<0.001), CCRT組的ypCR有29%, 其中pCR 在 adenocarcinoma (23%) versus squamous-cell carcinoma (49%) (P=0.008)
後來在2015年在lancet 發表長期追蹤的結果(median follow-up = 84.1 months), 確認不管是在adenocarcinoma or squamous carcinoma, 做neoadjuvant CCRT 都對OS 有幫助!
2021年又發表了十年長期追蹤結果(median follow-up:147 months), 發現neoadjuvant CRT 有比較好的 overall survival (hazard ratio [HR], 0.70; 95% CI, 0.55 to 0.89); 而且這個效應跟時間無關; 10年的overall survival benefit 是 38% v.s. 25%
表格整理如下:
MS = median overall survival; OS = overall survival
reference:
1. van Hagen, Pieter, et al. "Preoperative chemoradiotherapy for esophageal or junctional cancer." New England Journal of Medicine 366.22 (2012): 2074-2084.
2. Shapiro, Joel, et al. "Neoadjuvant chemoradiotherapy plus surgery versus surgery alone for oesophageal or junctional cancer (CROSS): long-term results of a randomised controlled trial." The lancet oncology 16.9 (2015): 1090-1098.
2019年5月26日 星期日
[食道癌] definitive CCRT
食道癌在治療上, 開刀算是主要治療, 但在不能開刀的病人身上, definitive CCRT 就會是主要的治療, 關於這個主題, 有幾篇經典的論文, 以下就來一一研讀:
1. RTOG8501: T1-3N0-1M0, SCC or adenoCa, 分成兩組, CRT(50Gy/25Fr+5-FU +cisplatin) v.s. RT alone(64Gy/32Fr), 5 yr OS 27%(CRT) v.s. 0%(RT), 10 yr OS, 20%(CRT), SCC 和 adenoCa 在結果上沒差
2. RTOG9405/INT0123: T1-4N0-1M0, SCC or adenoCa, 分成兩組, high dose CCRT(64.8Gy+5-FU +cisplatin) v.s. low dose CCRT(50.4Gy+5-FU +cisplatin), 在interim analysis後, 實驗就終止惹, 在high dose arm 有11個treatment-related death, 兩組在mean survival, 2-year OS, local regional failure沒有統計學上差別
reference:
1. Cooper, Jay S., et al. "Chemoradiotherapy of locally advanced esophageal cancer: long-term follow-up of a prospective randomized trial (RTOG 85-01)." Jama 281.17 (1999): 1623-1627.
2. Journal of Clinical Oncology 2002 20:5, 1167-1174
3. evidence-based radiation oncology
1. RTOG8501: T1-3N0-1M0, SCC or adenoCa, 分成兩組, CRT(50Gy/25Fr+5-FU +cisplatin) v.s. RT alone(64Gy/32Fr), 5 yr OS 27%(CRT) v.s. 0%(RT), 10 yr OS, 20%(CRT), SCC 和 adenoCa 在結果上沒差
2. RTOG9405/INT0123: T1-4N0-1M0, SCC or adenoCa, 分成兩組, high dose CCRT(64.8Gy+5-FU +cisplatin) v.s. low dose CCRT(50.4Gy+5-FU +cisplatin), 在interim analysis後, 實驗就終止惹, 在high dose arm 有11個treatment-related death, 兩組在mean survival, 2-year OS, local regional failure沒有統計學上差別
reference:
1. Cooper, Jay S., et al. "Chemoradiotherapy of locally advanced esophageal cancer: long-term follow-up of a prospective randomized trial (RTOG 85-01)." Jama 281.17 (1999): 1623-1627.
2. Journal of Clinical Oncology 2002 20:5, 1167-1174
3. evidence-based radiation oncology
[頭頸癌] 術後同步化放療論文整理
提到頭頸癌術後同步化放療, 就一定要提到兩篇文章, 分別是 EORTC 22931 和 RTOG9501
1. EORTC 22931: 頭頸癌開過刀(收案條件: pT3-4, pT1-2N2-3, oral cavity/oropharynx with levels IV/V LN involved, or T1-2N0-1 with ECE, margin+, LVI, or PNI ), 分成兩組, 一組接受放射治療(66Gy/33Fr)+化療(cisplatin 100mg/m^2 on days 1,22,43),另一組只接受放射治療(66Gy/33Fr), 結果為同步化放療組有比較好的OS, DFS, 5-yr local regional control, 但是grade 3,4 副作用比較多
2. RTOG9501: 頭頸癌開過刀(收案條件: ≥ 2 LNs, ECE, margin+), 分成兩組, 一組接受放射治療(60-66Gy in 2Gy/1Fr)+化療(cisplatin 100mg/m^2 on days 1,22,43),另一組只接受放射治療(60-66Gy in 2Gy/1Fr), 其結果為同步化放療組在DFS和2-yr local regional control比較好, 但是OS並沒有統計上差異; 後來在Red journal 有發表一篇長期追蹤的結果, 發現只有在ECE or margin positive 有 10yr-LRC的好處, 10yr-OS只有trend(p=0.07)
3. Bernier(2005): 這個作者把上面兩篇EORTC和RTOG9501做整合, 發現只有ECE and/or margin+的情況下, post-OP CRT 和 RT 相比可以改善 OS, DFS, LRC
reference:
1. Bernier, Jacques, et al. "Postoperative irradiation with or without concomitant chemotherapy for locally advanced head and neck cancer." New England Journal of Medicine 350.19 (2004): 1945-1952.
2. Cooper, Jay S., et al. "Postoperative concurrent radiotherapy and chemotherapy for high-risk squamous-cell carcinoma of the head and neck." New England Journal of Medicine 350.19 (2004): 1937-1944.
3. Cooper, Jay S., et al. "Long-term follow-up of the RTOG 9501/intergroup phase III trial: postoperative concurrent radiation therapy and chemotherapy in high-risk squamous cell carcinoma of the head and neck." International Journal of Radiation Oncology* Biology* Physics 84.5 (2012): 1198-1205.
4. Bernier, Jacques, et al. "Defining risk levels in locally advanced head and neck cancers: a comparative analysis of concurrent postoperative radiation plus chemotherapy trials of the EORTC (# 22931) and RTOG (# 9501)." Head & Neck: Journal for the Sciences and Specialties of the Head and Neck 27.10 (2005): 843-850.
5. Handbook of evidence-based radiation oncology 3rd edition
1. EORTC 22931: 頭頸癌開過刀(收案條件: pT3-4, pT1-2N2-3, oral cavity/oropharynx with levels IV/V LN involved, or T1-2N0-1 with ECE, margin+, LVI, or PNI ), 分成兩組, 一組接受放射治療(66Gy/33Fr)+化療(cisplatin 100mg/m^2 on days 1,22,43),另一組只接受放射治療(66Gy/33Fr), 結果為同步化放療組有比較好的OS, DFS, 5-yr local regional control, 但是grade 3,4 副作用比較多
2. RTOG9501: 頭頸癌開過刀(收案條件: ≥ 2 LNs, ECE, margin+), 分成兩組, 一組接受放射治療(60-66Gy in 2Gy/1Fr)+化療(cisplatin 100mg/m^2 on days 1,22,43),另一組只接受放射治療(60-66Gy in 2Gy/1Fr), 其結果為同步化放療組在DFS和2-yr local regional control比較好, 但是OS並沒有統計上差異; 後來在Red journal 有發表一篇長期追蹤的結果, 發現只有在ECE or margin positive 有 10yr-LRC的好處, 10yr-OS只有trend(p=0.07)
3. Bernier(2005): 這個作者把上面兩篇EORTC和RTOG9501做整合, 發現只有ECE and/or margin+的情況下, post-OP CRT 和 RT 相比可以改善 OS, DFS, LRC
reference:
1. Bernier, Jacques, et al. "Postoperative irradiation with or without concomitant chemotherapy for locally advanced head and neck cancer." New England Journal of Medicine 350.19 (2004): 1945-1952.
2. Cooper, Jay S., et al. "Postoperative concurrent radiotherapy and chemotherapy for high-risk squamous-cell carcinoma of the head and neck." New England Journal of Medicine 350.19 (2004): 1937-1944.
3. Cooper, Jay S., et al. "Long-term follow-up of the RTOG 9501/intergroup phase III trial: postoperative concurrent radiation therapy and chemotherapy in high-risk squamous cell carcinoma of the head and neck." International Journal of Radiation Oncology* Biology* Physics 84.5 (2012): 1198-1205.
4. Bernier, Jacques, et al. "Defining risk levels in locally advanced head and neck cancers: a comparative analysis of concurrent postoperative radiation plus chemotherapy trials of the EORTC (# 22931) and RTOG (# 9501)." Head & Neck: Journal for the Sciences and Specialties of the Head and Neck 27.10 (2005): 843-850.
5. Handbook of evidence-based radiation oncology 3rd edition
[淋巴癌] Hodgkin lymphoma 相關整理
1. 流行病學: 雙峰分佈, 25-30 以及 75-80
2. 組織學分類:
(1) Classical (佔95%): 特色為在發炎背景下有Reed-Sternberg cell (binucleate B cells, CD15+, CD30+), 又可分為四種
a. nodular sclerosis
b. mixed cellularity
c. lymphocyte rich
d. lymphocyte depleted
(2) Nodular lymphocyte predominant Hodgkin lymphoma(NLPHL, 5%): 其特色為lymphocyte-predominant cells (popcorn cell), CD15-,CD30-,CD45+,CD20+
3. 臨床表現: 大約80%有頸部淋巴結侵犯, 有50%有縱膈腔疾病, 大概有1/3的病人有B symptom(發燒,夜汗(night sweat), 過去六個月體重下降大於10%)
4. 分期: 1971就提出的Ann arbor分期, 以及後來WHO有新的分期方法; NCCN的分期是用 Ann Harbor, 表列如下:
2. 組織學分類:
(1) Classical (佔95%): 特色為在發炎背景下有Reed-Sternberg cell (binucleate B cells, CD15+, CD30+), 又可分為四種
a. nodular sclerosis
b. mixed cellularity
c. lymphocyte rich
d. lymphocyte depleted
(2) Nodular lymphocyte predominant Hodgkin lymphoma(NLPHL, 5%): 其特色為lymphocyte-predominant cells (popcorn cell), CD15-,CD30-,CD45+,CD20+
3. 臨床表現: 大約80%有頸部淋巴結侵犯, 有50%有縱膈腔疾病, 大概有1/3的病人有B symptom(發燒,夜汗(night sweat), 過去六個月體重下降大於10%)
4. 分期: 1971就提出的Ann arbor分期, 以及後來WHO有新的分期方法; NCCN的分期是用 Ann Harbor, 表列如下:
Stage I: 侵犯到單一淋巴區域(stage I) or 單一淋巴外器官或是區域(stage IE)
Stage II: 侵犯到橫膈膜同側兩個以上的淋巴區域(stage II) or 單一淋巴外器官或是區域以及其附屬淋巴結 +/- 橫膈膜同側的其他淋巴區域 (IIE)
侵犯淋巴結區域的數量可以標在下標, 比如說侵犯三個區域, 寫成 II3
Stage III: 侵犯到橫膈膜雙側的淋巴區域(III), 可以伴隨著侵犯到附屬的淋巴外器官或是區域(IIIE), 侵犯到脾臟(IIIS), or 兩個都有(IIIE+S)
Stage IV: Disseminated(multifocal) 侵犯一個以上的淋巴外器官, 加減伴隨的淋巴結侵犯; 或是單一的淋巴外器官侵犯加上遠處淋巴侵犯
此外註解也常寫 A, B, X
A: no B symptom
B: B symptom => Unexplained fever >38 Celsius degree; drenching night sweats; weight loss >10%(診斷前六個月內)
X: bulky disease
5. 治療方面: 主要都是先用化療, 之後再看治療反應決定後續治療, 在化療方面, 有許多regimen可以選, 常見的有ABVD.
6. 放射治療技術: ILROG(international lymphoma radiation oncology group)有推出治療準則, 目前主流是involved site RT(介在involved node RT 和 involved field RT 之間)
reference:
1. radiation oncology a question based review
2. https://www.ilrog.org/main-st
3. Perez and Brady's radiation oncology 7th edition
5. 治療方面: 主要都是先用化療, 之後再看治療反應決定後續治療, 在化療方面, 有許多regimen可以選, 常見的有ABVD.
6. 放射治療技術: ILROG(international lymphoma radiation oncology group)有推出治療準則, 目前主流是involved site RT(介在involved node RT 和 involved field RT 之間)
reference:
1. radiation oncology a question based review
2. https://www.ilrog.org/main-st
3. Perez and Brady's radiation oncology 7th edition
2019年5月25日 星期六
[子宮頸癌] 術後是否需要放射治療
在子宮頸癌早期的治療裡, 手術往往都是會先被考慮的選項, 至於手術後是否需要放射治療, 有一篇經典的研究(GOG92/ RTOG8706), 以及從這篇研究中整理出來的準則, Sedlis criteria, 以下就來仔細詳讀吧!
實驗設計如下: 子宮頸癌病人, stage IB, 接受過"radical hysterectomy", margin negative, node negative, risk factor 三個裡面有兩個以上(LVSI(+), tumor >4cm, >1/3 stromal invasion), 分成兩組, 一組接受放射治療(WPRT, 46-50.4Gy), 另外一組觀察, RT 在統計上顯著減少recurrence risk by 46% (hazard ratio = 0.54, 90% CI = 0.35 to 0.81, p = 0.007), RT在OS尚有改善, 但未達統計學上顯著意義 (HR = 0.70, 90% CI = 0.45 to 1.05, p = 0.074); 後來在red journal 發表長期追蹤的結果也是RT 在統計上顯著減少recurrence risk, 但在OS尚未達顯著意義
從這個研究裡, 出現了一個很有名的準則, 被稱為 Sedlis criteria, 子宮頸癌接受過radical hysterectomy後, 需要做放射治療的條件如下:
reference:
1. Sedlis, Alexander, et al. "A randomized trial of pelvic radiation therapy versus no further therapy in selected patients with stage IB carcinoma of the cervix after radical hysterectomy and pelvic lymphadenectomy: A Gynecologic Oncology Group Study." Gynecologic oncology 73.2 (1999): 177-183.
2. Rotman, Marvin, et al. "A phase III randomized trial of postoperative pelvic irradiation in Stage IB cervical carcinoma with poor prognostic features: follow-up of a gynecologic oncology group study." International Journal of Radiation Oncology* Biology* Physics 65.1 (2006): 169-176.
3. NCCN guildeline
實驗設計如下: 子宮頸癌病人, stage IB, 接受過"radical hysterectomy", margin negative, node negative, risk factor 三個裡面有兩個以上(LVSI(+), tumor >4cm, >1/3 stromal invasion), 分成兩組, 一組接受放射治療(WPRT, 46-50.4Gy), 另外一組觀察, RT 在統計上顯著減少recurrence risk by 46% (hazard ratio = 0.54, 90% CI = 0.35 to 0.81, p = 0.007), RT在OS尚有改善, 但未達統計學上顯著意義 (HR = 0.70, 90% CI = 0.45 to 1.05, p = 0.074); 後來在red journal 發表長期追蹤的結果也是RT 在統計上顯著減少recurrence risk, 但在OS尚未達顯著意義
從這個研究裡, 出現了一個很有名的準則, 被稱為 Sedlis criteria, 子宮頸癌接受過radical hysterectomy後, 需要做放射治療的條件如下:
LVSI
|
Stromal invasion
|
Tumor size(用摸的)
|
+
|
Deep 1/3
|
any
|
+
|
Middle 1/3
|
>=2 cm
|
+
|
Superficial 1/3
|
>=5cm
|
-
|
Middle or deep
1/3
|
>=4cm
|
reference:
1. Sedlis, Alexander, et al. "A randomized trial of pelvic radiation therapy versus no further therapy in selected patients with stage IB carcinoma of the cervix after radical hysterectomy and pelvic lymphadenectomy: A Gynecologic Oncology Group Study." Gynecologic oncology 73.2 (1999): 177-183.
2. Rotman, Marvin, et al. "A phase III randomized trial of postoperative pelvic irradiation in Stage IB cervical carcinoma with poor prognostic features: follow-up of a gynecologic oncology group study." International Journal of Radiation Oncology* Biology* Physics 65.1 (2006): 169-176.
3. NCCN guildeline
2019年5月22日 星期三
[膀胱癌] Muscle invasive bladder cancer
膀胱癌在預後上有一個很重要的因子, 就是是否有肌肉層的侵犯, 一但有肌肉層侵犯, 在AJCC分期上就至少是T2, 預後就相對不好
其治療方式, 標準的是radical cystectomy(男生: 移除膀胱和攝護腺;女生: 移除膀胱+子宮 ), 然而在特定病人可以考慮做bladder preservation, 其中最常用的方式被稱為Trimodality therapy(TMT),其意思為TURBT盡量刮除,之後再做CRT. 關於MIBC治療方法的研究很多,以下一一來整理
1. BC2001(NEJM2012): 共360個病人, 實驗設計為partial 2*2 factorial design
chemotherapy/RT v.s. RT alone,
whole bladder RT v.s. modified radiotherapy to uninvolved bladder
其中chemotherapy 是 5-FU+mitomycin
radiation therapy 是 64Gy/32Fr or 55Gy/20Fr
其結果為2 year locoregional DFS為chemo/RT比較好(67% v.s. 54%), 5ys-OS 和 late effect 在兩組沒有統計上差別

上面是比較chemoRT v.s. RT, 不過這是個partial 2*2 factorial design, 所以還可以繼續比較whole bladder RT v.s. modified radiotherapy to uninvolved bladder, 其結果發表在 2013的 red journal(連結點此)
所謂的modified radiotherapy to uninvolved bladder指的是腫瘤接受到full dose, 其他部分接受80%的dose
結果是 two year cumulative RTOG grade 3/4 toxicity:13% ,兩組的副作用在統計上沒差, local regional relapse 是用non-inferiority design, 其結果統計上無法正式下結論
reference:
1. James, Nicholas D., et al. "Radiotherapy with or without chemotherapy in muscle-invasive bladder cancer." New England Journal of Medicine 366.16 (2012): 1477-1488.
2. Huddart, Robert A., et al. "Randomized noninferiority trial of reduced high-dose volume versus standard volume radiation therapy for muscle-invasive bladder cancer: results of the BC2001 trial (CRUK/01/004)." International Journal of Radiation Oncology* Biology* Physics 87.2 (2013): 261-269.
其治療方式, 標準的是radical cystectomy(男生: 移除膀胱和攝護腺;女生: 移除膀胱+子宮 ), 然而在特定病人可以考慮做bladder preservation, 其中最常用的方式被稱為Trimodality therapy(TMT),其意思為TURBT盡量刮除,之後再做CRT. 關於MIBC治療方法的研究很多,以下一一來整理
1. BC2001(NEJM2012): 共360個病人, 實驗設計為partial 2*2 factorial design
chemotherapy/RT v.s. RT alone,
whole bladder RT v.s. modified radiotherapy to uninvolved bladder
其中chemotherapy 是 5-FU+mitomycin
radiation therapy 是 64Gy/32Fr or 55Gy/20Fr
其結果為2 year locoregional DFS為chemo/RT比較好(67% v.s. 54%), 5ys-OS 和 late effect 在兩組沒有統計上差別

上面是比較chemoRT v.s. RT, 不過這是個partial 2*2 factorial design, 所以還可以繼續比較whole bladder RT v.s. modified radiotherapy to uninvolved bladder, 其結果發表在 2013的 red journal(連結點此)
所謂的modified radiotherapy to uninvolved bladder指的是腫瘤接受到full dose, 其他部分接受80%的dose
結果是 two year cumulative RTOG grade 3/4 toxicity:13% ,兩組的副作用在統計上沒差, local regional relapse 是用non-inferiority design, 其結果統計上無法正式下結論
reference:
1. James, Nicholas D., et al. "Radiotherapy with or without chemotherapy in muscle-invasive bladder cancer." New England Journal of Medicine 366.16 (2012): 1477-1488.
2. Huddart, Robert A., et al. "Randomized noninferiority trial of reduced high-dose volume versus standard volume radiation therapy for muscle-invasive bladder cancer: results of the BC2001 trial (CRUK/01/004)." International Journal of Radiation Oncology* Biology* Physics 87.2 (2013): 261-269.
2019年5月20日 星期一
[腦瘤] WHO 2016分類
腦瘤(brain tumor)的分類標準由WHO在2016年更新, 之前的分類方法只看組織學型態來做分類, 新版分期多考慮了基因和影像特徵
組織學特徵主要是看這四個: nuclear atypia, cellularity and mitosis, endothelial proliferation, necrosis
WHO grade I: no factors present
WHO grade II: atypia
WHO grade III: atypia, mitoses
WHO grade IV: endothelial proliferation or necrosis
先來看glioma 分類(grade I, II 被稱為low-grade glioma; grade III,IV 被稱為 high-grade glioma):
WHO grade I: pilocytic astrocytoma, subependymal giant cell tumor
WHO grade II: diffuse astrocytoma, oligodendroglioma with IDH mutant/1p19q co-deleted, oligostrocytoma
WHO grade III: anaplastic astrocytoma(AA), anaplastic olidendroglioma(AO), anaplastic oligoastrocytoma(AOA)
WHO grade IV: GBM
reference:
1. handbook of evidence-based radiation oncology
2. radiation oncology a question based review
組織學特徵主要是看這四個: nuclear atypia, cellularity and mitosis, endothelial proliferation, necrosis
WHO grade I: no factors present
WHO grade II: atypia
WHO grade III: atypia, mitoses
WHO grade IV: endothelial proliferation or necrosis
先來看glioma 分類(grade I, II 被稱為low-grade glioma; grade III,IV 被稱為 high-grade glioma):
WHO grade I: pilocytic astrocytoma, subependymal giant cell tumor
WHO grade II: diffuse astrocytoma, oligodendroglioma with IDH mutant/1p19q co-deleted, oligostrocytoma
WHO grade III: anaplastic astrocytoma(AA), anaplastic olidendroglioma(AO), anaplastic oligoastrocytoma(AOA)
WHO grade IV: GBM
reference:
1. handbook of evidence-based radiation oncology
2. radiation oncology a question based review
[乳癌] hypofractionation相關論文整理
乳癌因為 $\alpha/\beta$ 小, 所以從radiobiology的觀點來看, hypofractionation自然就會是一個可考慮的選項, 因此這方面的臨床試驗也非常多, 以下是相關論文整理:
1. START-A: 英國研究, 收案條件為乳癌術後病人, pT1-3a pN0-1 M0, 50Gy/25Fr v.s. 39Gy/13Fr or 41.6Gy/13Fr, 實驗組和對照組的治療時間都是五周, 結果如下: 5-year local-regional relapse rates, 41.6Gy 和 50 Gy 相比是 0.2% (95% CI −1.3% to 2.6%), 39Gy 和 50Gy相比是 0·9% (95% CI −0·8% to 3·7%) ; 39Gy 和 50 Gy相比, late adverse effect 的發生比率比較低; $\alpha/\beta$ 在腫瘤控制方面是 4·6 Gy (95% CI 1·1–8·1) , 在 late change in breast appearance (photographic) 是 3·4 Gy (95% CI 2·3–4·5).
2. START-B: 英國研究, 收案條件為乳癌術後病人, pT1-3a pN0-1 M0, 50Gy/25Fr (治療五周) v.s. 40Gy/15Fr (治療三周), 追蹤年份中位數是 6·0 年 (IQR 5·0–6·2), 40 Gy組的 the rate of local-regional tumour relapse at 5 years 是 2·2% (95% CI 1·3–3·1), 50Gy組是 3·3% (95% CI 2·2 to 4·5), 40Gy的late adverse effects比50Gy少 (photographic and patient self-assessments)
3. canadian trial of hypofractionation: 加拿大研究, 收案條件為接受過BCS, pN0, 50Gy/25Fr v.s. 42.5Gy/16Fr, no boost, 10yr LR(6.2% v.s. 6.7%), DFS, OS, good/excellent cosmetic outcome 都沒有統計學上差別
4. RMH/GOC trial: 也是比較hypofractionation 跟coventional fractionation, breast cancer 接受手術, tumor stage I-III with at least one lymph node, 39Gy/13Fr, 42.9Gy/13Fr, 50Gy/25Fr, 去做比較, 治療時間是五周, 結果發現十年後同側乳房復發是 12.1% (95% CI 8.8-15.5) in the 50 Gy group, 14.8% (11.2-18.3) in the 39 Gy group, and 9.6% (6.7-12.6) in the 42.9 Gy group (difference between 39 Gy and 42.9 Gy groups, chi square test, p=0.027).
reference:
1. Trialists' Group, The START. "The UK Standardisation of Breast Radiotherapy (START) Trial A of radiotherapy hypofractionation for treatment of early breast cancer: a randomised trial." The lancet oncology 9.4 (2008): 331-341.
2. Bentzen, S. M., et al. "The UK Standardisation of Breast Radiotherapy (START) Trial B of radiotherapy hypofractionation for treatment of early breast cancer: a randomised trial." Lancet (London, England) 371.9618 (2008): 1098-1107.
3. Whelan, Timothy J., et al. "Long-term results of hypofractionated radiation therapy for breast cancer." New England Journal of Medicine 362.6 (2010): 513-520.
4. handbook of evidence-based radiation oncology
5. Kim, Kyung Su, et al. "Hypofractionated whole breast irradiation: new standard in early breast cancer after breast-conserving surgery." Radiation oncology journal 34.2 (2016): 81. (open access)
1. START-A: 英國研究, 收案條件為乳癌術後病人, pT1-3a pN0-1 M0, 50Gy/25Fr v.s. 39Gy/13Fr or 41.6Gy/13Fr, 實驗組和對照組的治療時間都是五周, 結果如下: 5-year local-regional relapse rates, 41.6Gy 和 50 Gy 相比是 0.2% (95% CI −1.3% to 2.6%), 39Gy 和 50Gy相比是 0·9% (95% CI −0·8% to 3·7%) ; 39Gy 和 50 Gy相比, late adverse effect 的發生比率比較低; $\alpha/\beta$ 在腫瘤控制方面是 4·6 Gy (95% CI 1·1–8·1) , 在 late change in breast appearance (photographic) 是 3·4 Gy (95% CI 2·3–4·5).
2. START-B: 英國研究, 收案條件為乳癌術後病人, pT1-3a pN0-1 M0, 50Gy/25Fr (治療五周) v.s. 40Gy/15Fr (治療三周), 追蹤年份中位數是 6·0 年 (IQR 5·0–6·2), 40 Gy組的 the rate of local-regional tumour relapse at 5 years 是 2·2% (95% CI 1·3–3·1), 50Gy組是 3·3% (95% CI 2·2 to 4·5), 40Gy的late adverse effects比50Gy少 (photographic and patient self-assessments)
3. canadian trial of hypofractionation: 加拿大研究, 收案條件為接受過BCS, pN0, 50Gy/25Fr v.s. 42.5Gy/16Fr, no boost, 10yr LR(6.2% v.s. 6.7%), DFS, OS, good/excellent cosmetic outcome 都沒有統計學上差別
4. RMH/GOC trial: 也是比較hypofractionation 跟coventional fractionation, breast cancer 接受手術, tumor stage I-III with at least one lymph node, 39Gy/13Fr, 42.9Gy/13Fr, 50Gy/25Fr, 去做比較, 治療時間是五周, 結果發現十年後同側乳房復發是 12.1% (95% CI 8.8-15.5) in the 50 Gy group, 14.8% (11.2-18.3) in the 39 Gy group, and 9.6% (6.7-12.6) in the 42.9 Gy group (difference between 39 Gy and 42.9 Gy groups, chi square test, p=0.027).
reference:
1. Trialists' Group, The START. "The UK Standardisation of Breast Radiotherapy (START) Trial A of radiotherapy hypofractionation for treatment of early breast cancer: a randomised trial." The lancet oncology 9.4 (2008): 331-341.
2. Bentzen, S. M., et al. "The UK Standardisation of Breast Radiotherapy (START) Trial B of radiotherapy hypofractionation for treatment of early breast cancer: a randomised trial." Lancet (London, England) 371.9618 (2008): 1098-1107.
3. Whelan, Timothy J., et al. "Long-term results of hypofractionated radiation therapy for breast cancer." New England Journal of Medicine 362.6 (2010): 513-520.
4. handbook of evidence-based radiation oncology
5. Kim, Kyung Su, et al. "Hypofractionated whole breast irradiation: new standard in early breast cancer after breast-conserving surgery." Radiation oncology journal 34.2 (2016): 81. (open access)
6. Owen JR, Ashton A, Bliss JM, et al. Effect of radiotherapy fraction size on tumour control in patients with early-stage breast cancer after local tumour excision: long-term results of a randomised trial [published correction appears in Lancet Oncol. 2006 Aug;7(8):620]. Lancet Oncol. 2006;7(6):467-471. doi:10.1016/S1470-2045(06)70699-4
[子宮內膜癌] 2009 FIGO stage
子宮內膜癌的分期很久沒更新惹,目前使用的版本是FIGO2009,小弟就來稍微整理一下,值得注意的是子宮內膜癌的分期是手術分期, 因為子宮內膜癌的標準治療就是分期手術(staging operation)
P.S. positive cytology 不影響分期
reference:
1. FIGO CANCER REPORT 2018
分期
|
描述
|
I
|
腫瘤只侷限在子宮
|
IA
|
侷限在子宮內膜或是侵犯子宮肌層小於一半(包括侵犯到內子宮頸腺體)
|
IB
|
侵犯子宮肌層大於等於一半
|
II
|
腫瘤侵犯到子宮頸基質,但還沒侵犯出子宮
|
III
|
|
IIIA
|
腫瘤侵犯到子宮漿膜或是附屬器官
|
IIIB
|
腫瘤侵犯到陰道或是parametrium
|
IIIC
|
淋巴結轉移
|
IIIC1
|
骨盆腔淋巴結轉移
|
IIIC2
|
主動脈旁淋巴結轉移
|
IV
|
|
IVA
|
侵犯到膀胱或是腸道黏膜
|
IVB
|
跑到遠處器官
|
P.S. positive cytology 不影響分期
reference:
1. FIGO CANCER REPORT 2018
2019年5月19日 星期日
[radiobiology] fractionation
在放射治療技術裡, 有一個非常迷人的主題, 就是利用改變劑量, 治療次數和總治療時間, 來觀察治療效果以及正常組織副作用的變化, 先來認識幾個名詞
1. conventional fractionation: 標準的放射治療劑量給法, 1 fraction 給 1.8Gy-2.0Gy, 一天一次, 一周給五天, 總共給多少劑量要看腫瘤和周遭正常組織來定
2. hyperfractionation: 1 fraction 給低於1.8Gy的劑量, 給的次數增加
3. hypofractionation: 1 fraction 給大於2.0Gy的劑量, 給的次數減少
那實際上上述幾種治療策略對正常組織會有甚麼影響呢? 這就是重點惹
大家都知道正常組織可以簡單分成early responding tissue 和 late responding tissue, 其中early responding tissue 會受到總治療時間(total treatment time)和 fraction size(單次治療劑量)的影響; 而late responding tissue主要是受到fraction size的影響, 原理很簡單, 解釋如下:
首先是治療時間的部分, 大家都知道early responding tissue,例如皮膚, 其實在放射治療一段時間後, 就會開始細胞增生, 因此分次治療時間拉得越長, 對early responding tissue的保護會越好; 但是late responding tissue在正常的放射治療次數裡,是不可能會出現細胞增生的, 因此治療時間對late responding tissue是沒有影響的
再來是fraction size的部分, 這部分就要回歸到LQ model惹, early responding tissue 的 $\alpha/\beta$ 比較大, 而late responding tissue 的 $\alpha/\beta$ 相對小, 所以fraction size變大, 對late responding tissue的影響比較大
所以hypofractionation在臨床上對$\alpha/\beta$小的腫瘤,例如breast cancer(相關論文整理), prostate cancer是有幫助的(因為這些腫瘤的$\alpha/\beta$常常都比周遭正常組織還小); 另外就是fraction size增加容易增加late complication, 但是如果是palliative的情況,可能病人剩餘生命並不足以等到late complication發生, 因此也可以使用hypofractionation, 例如臨床常見的whole brain RT, bone mets RT....
至於hyperfractionation 拉長治療時間, 對early responding tissue的保護比較好, 降低fraction size對late responding tissue的保護也會更好, 但是治療時間會拉的很長,而且許多腫瘤,特別是頭頸部癌症會有所謂的acclerated repopulation, 也就是治療時間拉長, 大概28天, 腫瘤反而會加速生長, 因此治療時間拉太長也不會是好事....
reference:
1. radiobiology for the radiologist 8th edition
2. basic clinical radiobiology 5th edition
1. conventional fractionation: 標準的放射治療劑量給法, 1 fraction 給 1.8Gy-2.0Gy, 一天一次, 一周給五天, 總共給多少劑量要看腫瘤和周遭正常組織來定
2. hyperfractionation: 1 fraction 給低於1.8Gy的劑量, 給的次數增加
3. hypofractionation: 1 fraction 給大於2.0Gy的劑量, 給的次數減少
那實際上上述幾種治療策略對正常組織會有甚麼影響呢? 這就是重點惹
大家都知道正常組織可以簡單分成early responding tissue 和 late responding tissue, 其中early responding tissue 會受到總治療時間(total treatment time)和 fraction size(單次治療劑量)的影響; 而late responding tissue主要是受到fraction size的影響, 原理很簡單, 解釋如下:
首先是治療時間的部分, 大家都知道early responding tissue,例如皮膚, 其實在放射治療一段時間後, 就會開始細胞增生, 因此分次治療時間拉得越長, 對early responding tissue的保護會越好; 但是late responding tissue在正常的放射治療次數裡,是不可能會出現細胞增生的, 因此治療時間對late responding tissue是沒有影響的
再來是fraction size的部分, 這部分就要回歸到LQ model惹, early responding tissue 的 $\alpha/\beta$ 比較大, 而late responding tissue 的 $\alpha/\beta$ 相對小, 所以fraction size變大, 對late responding tissue的影響比較大
所以hypofractionation在臨床上對$\alpha/\beta$小的腫瘤,例如breast cancer(相關論文整理), prostate cancer是有幫助的(因為這些腫瘤的$\alpha/\beta$常常都比周遭正常組織還小); 另外就是fraction size增加容易增加late complication, 但是如果是palliative的情況,可能病人剩餘生命並不足以等到late complication發生, 因此也可以使用hypofractionation, 例如臨床常見的whole brain RT, bone mets RT....
至於hyperfractionation 拉長治療時間, 對early responding tissue的保護比較好, 降低fraction size對late responding tissue的保護也會更好, 但是治療時間會拉的很長,而且許多腫瘤,特別是頭頸部癌症會有所謂的acclerated repopulation, 也就是治療時間拉長, 大概28天, 腫瘤反而會加速生長, 因此治療時間拉太長也不會是好事....
reference:
1. radiobiology for the radiologist 8th edition
2. basic clinical radiobiology 5th edition
[口腔癌] AJCC 8 分期
口腔癌分期, 看書想要懂的話, 真的超痛苦, 因為AJCC 在2016年發表了第八版最新分期, 然而書中在口腔癌的部份錯誤蠻多的, 因此在2018年5月有做更新, 然而許多書籍和網站並沒有因此更正, 所以大家會發現每本寫得不一樣, 以下是小弟我去AJCC網站把勘誤後的版本整理下來,跟大家分享
p.s. DOI = depth of invasion, not tumor thickness
p.s. DOI為腫瘤侵犯深度,大家可以簡單思考一下就知道, 要準確知道DOI要靠病理(其實從影像上也可以大概判斷DOI(reference 5)),口腔癌大部份都會開刀,因此T的分期可能開刀前和開刀後不一樣
P.S. 上面的T4a 有提到corticol bone, 幫大家回憶一下組織學, 組織學裡面提到骨頭可以分成 compact(corticol) bone 和 trabecular bone, 下面是圖解:

外層的叫做corticol bone, 又叫做compact bone, 意指為質地比較緊密, 而內層叫做trabecular bone, 質地比較鬆散, 內部含有骨髓和血管
因為對於T4a的定義還是覺得有不清楚的地方, 因此去信詢問AJCC committee, 得到回應如下: corticol bone的erosion意指為看到骨頭表面有空掉的地方; 而corticol bone invasion 代表結構被破壞, 如果分期上有不清楚的地方, 以較低的分期為主
pathological N stage:
N1: 同側單顆, ≤ 3cm, ENE(-)
N2a: 同側單顆, ≤ 3cm, ENE(+) or 同側單顆, >3cm, ≤ 6cm, ENE(-)
N2b: 同側多顆, ≤ 6cm, ENE(-)
N2c: 雙側或對側, ≤ 6cm, ENE(-)
N3a: >6cm, ENE(-)
N3b: 同側單顆, > 3cm, ENE(+) or 多顆, ENE(+) or 對側單顆, ENE(+)
M:
M0: 沒有遠端轉移
M1: 有遠端轉移
prognostic stage:
M1 => stage IVC
reference:
T stage:
T1: tumor ≤ 2cm with DOI ≤ 5mm
T2: tumor ≤ 2cm with DOI > 5mm or tumor > 2cm and ≤ 4cm with DOI ≤ 10mm
T3: tumor > 2cm and ≤ 4cm with DOI > 10mm or tumor > 4cm with DOI ≤ 10mm
T4a: moderately advanced local disease
tumor > 4 cm with DOI > 10 mm or tumor invades adjacent structures only (e.g., through cortical bone of the mandible or maxilla or involves the maxillary sinus or skin of the face)
Note: Superficial erosion of bone/tooth socket (alone) by a gingival primary is not sufficient to classify a tumor as T4."
T4b: very advanced local disease
tumor invades masticator space, pterygoids plates, or skull space and/or encases the internal carotid artery
p.s. DOI = depth of invasion, not tumor thickness
p.s. DOI為腫瘤侵犯深度,大家可以簡單思考一下就知道, 要準確知道DOI要靠病理(其實從影像上也可以大概判斷DOI(reference 5)),口腔癌大部份都會開刀,因此T的分期可能開刀前和開刀後不一樣
P.S. 上面的T4a 有提到corticol bone, 幫大家回憶一下組織學, 組織學裡面提到骨頭可以分成 compact(corticol) bone 和 trabecular bone, 下面是圖解:

外層的叫做corticol bone, 又叫做compact bone, 意指為質地比較緊密, 而內層叫做trabecular bone, 質地比較鬆散, 內部含有骨髓和血管
因為對於T4a的定義還是覺得有不清楚的地方, 因此去信詢問AJCC committee, 得到回應如下: corticol bone的erosion意指為看到骨頭表面有空掉的地方; 而corticol bone invasion 代表結構被破壞, 如果分期上有不清楚的地方, 以較低的分期為主
T 的部份可以用個簡表幫助記憶:

至於N的部分也是非常複雜,可以分成clinical和pathological
clinical N stage:
N1: 同側單顆, ≤ 3cm, ENE(-)
N2a: 同側單顆, >3cm, ≤ 6cm, ENE(-)
N2b: 同側多顆, ≤ 6cm, ENE(-)
N2c: 雙側或對側, ≤ 6cm, ENE(-)
N3a: >6cm, ENE(-)
N3b: 臨床上明顯有ENE(不能只靠影像,還要加上理學檢查支持)
P.S. ENE=extranodal extension

至於N的部分也是非常複雜,可以分成clinical和pathological
clinical N stage:
N1: 同側單顆, ≤ 3cm, ENE(-)
N2a: 同側單顆, >3cm, ≤ 6cm, ENE(-)
N2b: 同側多顆, ≤ 6cm, ENE(-)
N2c: 雙側或對側, ≤ 6cm, ENE(-)
N3a: >6cm, ENE(-)
N3b: 臨床上明顯有ENE(不能只靠影像,還要加上理學檢查支持)
P.S. ENE=extranodal extension
pathological N stage:
N1: 同側單顆, ≤ 3cm, ENE(-)
N2a: 同側單顆, ≤ 3cm, ENE(+) or 同側單顆, >3cm, ≤ 6cm, ENE(-)
N2b: 同側多顆, ≤ 6cm, ENE(-)
N2c: 雙側或對側, ≤ 6cm, ENE(-)
N3a: >6cm, ENE(-)
N3b: 同側單顆, > 3cm, ENE(+) or 多顆, ENE(+) or 對側單顆, ENE(+)
M:
M0: 沒有遠端轉移
M1: 有遠端轉移
prognostic stage:
N0
|
N1
|
N2
|
N3
|
|
T1
|
I
|
III
|
IVA
|
IVB
|
T2
|
II
|
III
|
IVA
|
IVB
|
T3
|
III
|
III
|
IVA
|
IVB
|
T4a
|
IVA
|
IVA
|
IVA
|
IVB
|
T4b
|
IVB
|
IVB
|
IVB
|
IVB
|
M1 => stage IVC
reference:
1. AJCC webiste
2. radiation oncology, a question-based review
3. Wheater's Functional Histology
4. Histology, a text and atlas
5. http://www.ajnr.org/content/ajnr/early/2018/08/30/ajnr.A5782.full.pdf
2. radiation oncology, a question-based review
3. Wheater's Functional Histology
4. Histology, a text and atlas
5. http://www.ajnr.org/content/ajnr/early/2018/08/30/ajnr.A5782.full.pdf
2019年5月18日 星期六
[放射治療技術] 醫用直線加速器
傳統的放射治療利用 60 Co當作射源, 其缺點為 60 Co會持續衰變, 隨著技術進步, 現今台灣的放射腫瘤科都使用直線加速器(Linear accelerator, 簡稱為Linac), 其原理為加速電子, 利用電子去撞擊金屬靶, 產生X光, 或是直接把電子打出來去治療病人, 以下就由我來詳細介紹直線加速器的原理以及結構吧!
先來看一下直線加速器的示意圖:

其中gantry, collimator, 和許多linac的table都可以旋轉, 如果把gantry的部分放大來看:

其作用原理如下: power supply 為能量提供者, 提供直流電(DC)給modulator, modulator 會形成pulse, 分別給magnetron(or kylstron) 以及electron gun, magnetron(or kylstron)會接收到pulse, 之後產生pulsed microwave, 再傳給accelerator tube, 拿來加速electron gun 傳入accelerator tube的電子, 如果是想要用x-ray治療病人的話,還會再把電子拿去撞擊金屬靶,進而產生光子,治療病人
p.s. 也不是所有的醫用直線加速器的gantry都可以旋轉, tomotherapy的gantry是固定的
p.s. 有一個臨床上常常搞混的概念, 就是大家常常會說這個直線加速器是幾MV的, 比如說常見有6MV的直線加速器, 單位不用MeV的原因是因為直線加速器產生的X光是bremsstrahlung, 其為連續能量的X ray, 並非單一能量
reference:
1. Clinical radiation oncology
2. Khan's the physics of radiation therapy 5th edition
先來看一下直線加速器的示意圖:

其中gantry, collimator, 和許多linac的table都可以旋轉, 如果把gantry的部分放大來看:

其作用原理如下: power supply 為能量提供者, 提供直流電(DC)給modulator, modulator 會形成pulse, 分別給magnetron(or kylstron) 以及electron gun, magnetron(or kylstron)會接收到pulse, 之後產生pulsed microwave, 再傳給accelerator tube, 拿來加速electron gun 傳入accelerator tube的電子, 如果是想要用x-ray治療病人的話,還會再把電子拿去撞擊金屬靶,進而產生光子,治療病人
p.s. 也不是所有的醫用直線加速器的gantry都可以旋轉, tomotherapy的gantry是固定的
p.s. 有一個臨床上常常搞混的概念, 就是大家常常會說這個直線加速器是幾MV的, 比如說常見有6MV的直線加速器, 單位不用MeV的原因是因為直線加速器產生的X光是bremsstrahlung, 其為連續能量的X ray, 並非單一能量
reference:
1. Clinical radiation oncology
2. Khan's the physics of radiation therapy 5th edition
2019年5月16日 星期四
[小兒腫瘤] 神經母細胞瘤(neuroblastoma)相關整理
1. 流行病學特性: 最常見的顱外小兒實體腫瘤
2. 好發位置: 最常見的是adrenal medulla(30-40%), 其次是在腹腔或骨盆腔的paraspinal ganglia (25%)
3. 遠處轉移: 超過70%的病人在診斷時已有轉移(如果發現轉移時,VMA/HVA>1.5的話,預後比較好)
4. 分期:
2. 好發位置: 最常見的是adrenal medulla(30-40%), 其次是在腹腔或骨盆腔的paraspinal ganglia (25%)
3. 遠處轉移: 超過70%的病人在診斷時已有轉移(如果發現轉移時,VMA/HVA>1.5的話,預後比較好)
4. 分期:
(1)INSS(international staging system) => 1993年, 過去常用
stage 1: 做過GTR(gross tumor resection), +/- microscopic residual tumor; ipsilateral adherent LN 可以有, 但是non-adherent LN 一定要沒有
5. 治療(based on COG risk group):
(1) low risk: 把腫瘤完全切除, 即使切不乾淨, 也不一定要進一步治療(一歲以下手術切除後要加上化療); 如果是4S 的話, 可以考慮觀察就好, 因為腫瘤有可能spontaneous regression
stage 1: 做過GTR(gross tumor resection), +/- microscopic residual tumor; ipsilateral adherent LN 可以有, 但是non-adherent LN 一定要沒有
stage 2A: 做過GTR(gross tumor resection), incomplete gross resection; ipsilateral non-adherent LN 沒有
stage 2B: 局部腫瘤, ipsilateral non-adherent LN 有, 但是對側淋巴結一定要沒有
stage 3: 不能手術的腫瘤, 或者是腫瘤跨過中線, 或者是對側淋巴結侵犯, 或者是中線腫瘤有兩側侵犯
stage 4: 遠端轉移
stage 4S: 小於一歲的stage 1,2病人, 雖已發生轉移, 但轉移僅限於骨髓(<10%),肝臟或皮膚 => 預後佳
stage 3: 不能手術的腫瘤, 或者是腫瘤跨過中線, 或者是對側淋巴結侵犯, 或者是中線腫瘤有兩側侵犯
stage 4: 遠端轉移
stage 4S: 小於一歲的stage 1,2病人, 雖已發生轉移, 但轉移僅限於骨髓(<10%),肝臟或皮膚 => 預後佳
=> 可以根據 INSS stage + Age + MYCN status + Shimada histology + DNA ploidy =>
去計算 COG risk groups (based on INSS stage), 會再分成以下三個risk group:
1. low risk
2. intermediate risk
3. high risk
(2) INRGSS stage:
(2) INRGSS stage:
L1
L2
M
MS
=> 可以依照 INRGSS +
=> 去計算 risk groups, 會再分成以下四個risk group:
1. very low risk
2. low risk
3. intermediate risk
4. high risk
5. 治療(based on COG risk group):
(1) low risk: 把腫瘤完全切除, 即使切不乾淨, 也不一定要進一步治療(一歲以下手術切除後要加上化療); 如果是4S 的話, 可以考慮觀察就好, 因為腫瘤有可能spontaneous regression
(2) intermediate risk: 先手術在做化療, 如果腫瘤太大, 可以考慮先做化療
(3) high risk:先給化療, 再做手術切除
reference:
1. radiation oncology management decisions 4th edition
(3) high risk:先給化療, 再做手術切除
reference:
1. radiation oncology management decisions 4th edition
2. ASTRO annual refresher course 2021
2019年5月12日 星期日
[乳癌] 術中放射治療
乳癌的術中放射治療, 其意義為在乳癌手術中, 進行一次性的術中放射治療(prepatholgy), 或是在術後確認病理分期的時候,再打開傷口把放射治療器具放入(postpathology), 利用一次的治療來節省病人的時間, 但成效究竟如何呢, 以下是相關論文整理
1. Targit-A: 為英國針對早期乳癌病人, 45歲以上, unifocal lesion, 排除lobular carcinoma, 利用50 KV x ray(orthovoltage)技術進行治療, 其劑量為20Gy/1Fr, 使用non-inferiority trial design, 其結果如下:
如果用subgroup分析5-year risk for Local recurrence的話:
prepathology v.s. EBRT: 2·1% vs 1·1% (p=0·31)
postpathology v.s. EBRT: 5·4% vs 1·7% (p=0·069)
結論: IORT 可以在prepathology的情況下, 被考慮當作體外放射治療的替代治療
JAMA oncology在2020年發表了長期追蹤的結果[3], 主要是針對post-pathology的部分, 發現在long-term (median = 9 yrs) mastectomy-free survival, distant disease-free survival, and overall survival 沒差, 但是locoregional recurrence, postpathology-IORT 還是比較高
1. Targit-A: 為英國針對早期乳癌病人, 45歲以上, unifocal lesion, 排除lobular carcinoma, 利用50 KV x ray(orthovoltage)技術進行治療, 其劑量為20Gy/1Fr, 使用non-inferiority trial design, 其結果如下:
接受乳房手術
|
Targit(single-dose
targeted intraoperative radiotherapy)
|
EBRT
|
5-year
risk for Local recurrence
(median follow-up: 2y5m)
|
3.3%
|
1.3%
|
p=0·042
|
||
breast cancer mortality
|
2.6%
|
1.9%
|
p=0.56
|
||
non-breast-cancer
deaths
|
1·4%
|
3·5%
|
p=0·0086
|
||
Overall mortality
|
3.9%
|
5.3%
|
p=0·099
|
||
grade 3 or 4
skin complications
|
4
|
13
|
p=0·029
|
||
prepathology v.s. EBRT: 2·1% vs 1·1% (p=0·31)
postpathology v.s. EBRT: 5·4% vs 1·7% (p=0·069)
結論: IORT 可以在prepathology的情況下, 被考慮當作體外放射治療的替代治療
JAMA oncology在2020年發表了長期追蹤的結果[3], 主要是針對post-pathology的部分, 發現在long-term (median = 9 yrs) mastectomy-free survival, distant disease-free survival, and overall survival 沒差, 但是locoregional recurrence, postpathology-IORT 還是比較高
BMJ 在 2020 年也發表了長期追蹤的結果, 主要是針對pre-pathology的部分, 結果發現 IORT 在 local control, mastectomy-free survival, distant disease-free survival, overall survival, and breast cancer mortality 都跟 EBRT 差不多, 在non-breast cancer mortality 方面來說還比較低
=> Targit-A 以結果來說, 比較傾向使用Pre-pathology, 如果因為某些因素使用post-pathology IORT的話, 就要付出local control 比較差的代價
2. Milan ELIOT trial:
reference:
1. Vaidya, Jayant S., et al. "Risk-adapted targeted intraoperative radiotherapy versus whole-breast radiotherapy for breast cancer: 5-year results for local control and overall survival from the TARGIT-A randomised trial." The Lancet 383.9917 (2014): 603-613.
2. Veronesi, Umberto, et al. "Intraoperative radiotherapy versus external radiotherapy for early breast cancer (ELIOT): a randomised controlled equivalence trial." The lancet oncology 14.13 (2013): 1269-1277.
2. Milan ELIOT trial:
接受乳房手術
|
IORT with
electron
|
WBRT+boost
|
Ipsilateral breast tumor
recurrence (IBTR) – 5 year event rate
|
4.4%
|
0.4%
|
Hazard ratio=9.3 [95% CI 3·3–26·3]
|
||
5-year overall
survival
|
96.8%
|
96.9%
|
p=0.56
|
||
Fewer skin side effect in IORT(p=0.0002)
|
||
reference:
1. Vaidya, Jayant S., et al. "Risk-adapted targeted intraoperative radiotherapy versus whole-breast radiotherapy for breast cancer: 5-year results for local control and overall survival from the TARGIT-A randomised trial." The Lancet 383.9917 (2014): 603-613.
2. Veronesi, Umberto, et al. "Intraoperative radiotherapy versus external radiotherapy for early breast cancer (ELIOT): a randomised controlled equivalence trial." The lancet oncology 14.13 (2013): 1269-1277.
4. Vaidya JS, Bulsara M, Baum M, et al. Long term survival and local control outcomes from single dose targeted intraoperative radiotherapy during lumpectomy (TARGIT-IORT) for early breast cancer: TARGIT-A randomised clinical trial. BMJ. 2020;370:m2836. Published 2020 Aug 19. doi:10.1136/bmj.m2836
訂閱:
文章 (Atom)
-
醫師選科 這個網頁主要目的是為了幫助 面對選科困惑的醫學系畢業生們 希望結果能對你/妳有幫助 測驗總共18題 點擊下面按鈕 馬上開始吧 Click Me! 跟病人建立長久關係 喜歡 還好 不喜歡 學習數學物理知識 喜歡 還好...
-
 在放射治療裡面, 有一個很基礎的概念, 就是在定義放射治療的範圍, 其中有所謂的 GTV, CTV, PTV的概念 1. GTV(gross tumor volume): 就是影像上(CT, MRI,echo...)或是肉眼,理學檢查能夠看到的腫瘤範圍 2. CTV(cli...
在放射治療裡面, 有一個很基礎的概念, 就是在定義放射治療的範圍, 其中有所謂的 GTV, CTV, PTV的概念 1. GTV(gross tumor volume): 就是影像上(CT, MRI,echo...)或是肉眼,理學檢查能夠看到的腫瘤範圍 2. CTV(cli... -
在放射物理教科書 Khan 裡面, 第二章主要討論Nuclear transformation, 這章的重點在於放射物質的衰變以及各種核反應(nuclear reaction) 首先要先了解radioactivity是甚麼, 中文翻譯為放射性, 意思是輻射從原子裡面釋放出來, 這...
